")
The Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA) became law on October 3, 2008, and took effect January 1, 2010. The MHPAEA requires that insurance plans and health insurers, who are providing both medical and surgical (M/S) coverage and mental health and substance use disorder (MH/SUD) coverage, prohibit discriminating between coverage offered for mental illness, serious mental illness, substance abuse, and other physical disorders and diseases.
In 2016, the Centers for Medicare and Medicaid Services (CMS) finalized a rule to strengthen access to mental health and substance use disorder services for people with Medicaid, Children’s Health Insurance Program (CHIP), or Alternative Benefit Plan (ABP) coverage. The rule requires that Medicaid, CHIP, and ABP Managed Care Plans not impose more restrictive benefit limitations on mental health and substance use disorder benefits than on medical and surgical benefits. In short, parity requires insurers to provide the same level of benefits for mental illness, serious mental
illness or substance abuse as for other physical disorders and diseases. These parity requirements include aggregate lifetime and annual dollar limits, financial requirements (e.g., co-payments), quantitative treatment limitations (e.g., visitation limits), and non-quantitative treatment limitations (e.g., utilization management policies and procedures).
Understanding the Issues and Implications
Although mental health parity compliance is a major focus for both state and federal regulators, many states have no parity regulations or their parity regulations are limited in scope. This means that most individuals with health care coverage encounter more difficulty and greater barriers to MH/SUD services than for other medical conditions. In addition, MH/SUD services often come with higher out of-pocket costs and narrower scopes of coverage for these benefits.
This is why states should determine if there are gaps in their mental health and substance abuse coverage when compared to medical and surgical coverage. Then states should ensure they understand the federal regulations and prepare effective implementation of the parity law.
If states do not implement policies that align with federal parity laws, there could be detrimental consequences for managed care members and their families. When claims are denied due to lack of MH/SUD coverage, members and their families are forced to go without treatment. Untreated mental health conditions can lead to higher health care costs, increased utilization, and poor medication adherence.
In fact, according to Mental Health America, studies show that “equalizing specialty behavioral health and general medical benefits will either not increase total health care expenses at all or will increase them by only a very modest amount of total healthcare premium The real cost lies in not treating behavioral health disorders.”1
Guidance from the Centers for Medicare & Medicaid Services
The Centers for Medicare & Medicaid Services (CMS) guidance includes guidance and specific parity compliance requirements for each managed care organization (MCO) providing services to members. For example, MCOs that have no certain aggregate or lifetime dollar limits M/S benefits also may not impose limits in kind on SUD benefits.2 Those that do impose a limit on at least two-thirds of all M/S benefits must either apply those limits to SUD benefits in a way that does not differentiate between the two or NOT include a limit on SUD that does not also exist on M/S benefits.2
Put another way, any benefits or limitations within M/S benefits must be similarly applied to those of SUD benefits, which may not be relatively more limited or restricted in terms of cost or services. Further, SUD benefits cannot be subject to separate cost-sharing standards or treatment limitations that apply only to these benefits. If requested, the provider must disclose standards for medical necessity determinations and reasons for denials related to MH/SUD benefits must be disclosed upon request.3
Oversight of Mental Health Parity Requirements
The Office of Inspector General (OIG) recently added ‘States’ and MCOs’ Compliance With Mental Health Parity Requirements’ to its work plan, intended for release in fiscal year 2023. The OIG will audit CMS’s oversight of States’ compliance with Federal parity requirements, including whether States and their MCOs conducted the required parity analyses and whether States ensured their MCOs complied with certain parity requirements for MH/SUD benefits.4
Additionally, the oversight of compliance with the mental health parity rules was evaluated by the General Accounting Office (GAO) in a report issued in December 2019. The GAO report discovered CMS’ oversight was limited to targeted reviews, ordinarily based on information it received, such as a consumer complaints rather than a comprehensive program.
CREATING PARITY
MHPAEA requires parity between medical/surgical benefits and mental health and substance use disorder. Here are just a few ways it seeks to accomplish parity:
- Lifetime or annual dollar limits for MH/SUD benefits cannot be greater than those for M/S benefits.
- Limitations on treatment scope (e.g., frequency of treatment, number of days) for MH/SUD benefits cannot be greater for than for M/S.
- Where a state parity law or mandate exists, “the Federal Parity law serves as the floor, and state laws must be enhanced to reach the federal floor.”5
Despite the simplicity in the MHPAEA, which seeks to correct imbalances and inequities, the underlying complexity can be difficult to dismantle so that the individual components can correctly be evaluated and addressed.
Stakeholders believe complaints are not a reliable indicator of the extent of noncompliance because consumers may not know about MH/SUD parity requirements or may have privacy concerns related to submitting a complaint. The GAO recommended CMS evaluate whether this approach created significant risks. CMS concurred with the recommendation and stated it would also evaluate whether seeking additional oversight authority and resources was necessary.6
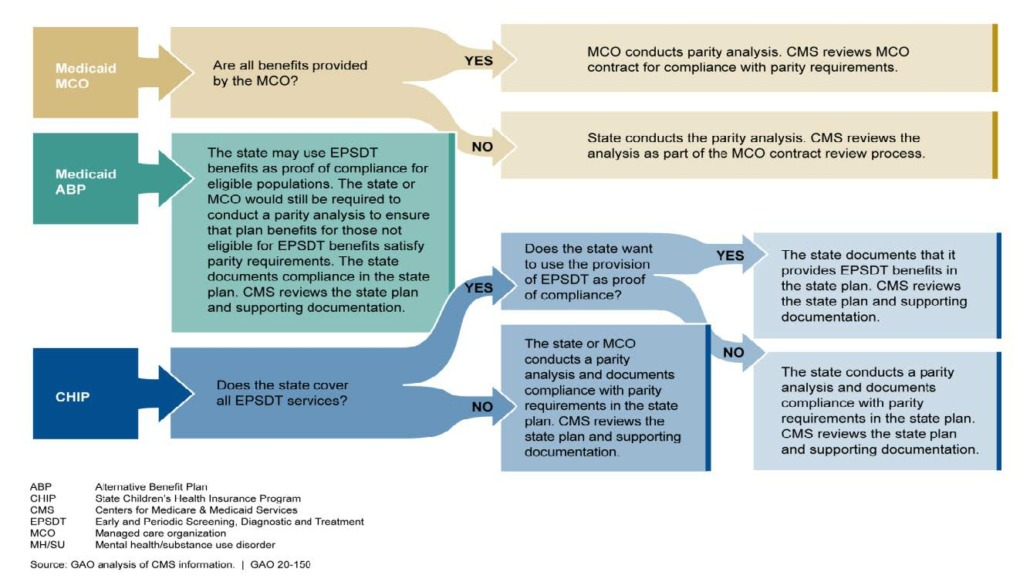
Understanding When the MCO or State Should Conduct the Parity Analysis
How We Can Help
Myers and Stauffer can help state agencies create a mental health parity strategy that is driven by our experience in Medicaid agency policy and operations consulting alongside our skill in financial and performance audits of Medicare and Medicaid managed care organizations. We can provide:
- Review of the current mental/behavioral health services policies and procedures.
- Development of a state-specific reporting tool.
- Assistance with the evaluation, oversight and monitoring of the health plan’s mental health parity data submissions to ensure compliance with the parity requirements under MHPAEA.
Managed Care: Regulatory Knowledge Combined with Tactical Skill. Since 2004, we have assisted our state clients with developing comprehensive monitoring processes for their managed care programs, including managed care oversight and consulting for more than 20 states and the federal government.
Consulting: Demonstrated Success: Health Care Transformation. Our team has provided consulting for some of the nation’s most innovative and effective health care delivery system and payment transformation initiatives. We have been involved in every phase of policy and program planning, implementation, operation, and evaluation. Often, our work involves the coordination of multiple concurrent reform efforts that we have successfully navigated in the past, which demonstrates our in-depth understanding of delivery system and payment transformation, quality programs and
measures, and evaluation of health outcomes. Stakeholders believe complaints are not a reliable indicator of the extent of noncompliance because consumers may not know about MH/SUD parity requirements or may have privacy concerns related to submitting a complaint. The GAO recommended CMS evaluate whether this approach created significant risks. CMS concurred with the
recommendation and stated it would also evaluate whether seeking additional oversight authority and resources was
necessary.6
1 https://www.mhanational.org/issues/issue-brief-parity.
2 https://www.ecfr.gov/current/title-42/chapter-IV/subchapter-C/part-438/subpart-K/section-438.905#p-438.905(b).
3 https://www.cms.gov/CCIIO/Programs-and-Initiatives/Other-Insurance-Protections/mhpaea_factsheet.
4 https://oig.hhs.gov/reports-and-publications/workplan/summary/wp-summary-0000710.asp
5 https://www.mhanational.org/issues/issue-brief-parity
6 ttps://www.gao.gov/products/gao-20-150.
| Michael Johnson, CPA, CFE (Member)
PH 404.524.9505 PH 866.758.3586 |
Stephen Fader, CFE (Senior Manager)
PH 404.524.9049 PH 866.758.3586 |
Kelly Horan
(Senior Manager) PH 303.694.3605 PH 866.758.3586
|
Savombi Fields, CFE, CPC-P (Senior Manager)
PH 404.524.9507 PH 866.7585.3586 |